This is a guest post by Katie Dahlhausen, a PhD Student in my lab.
Koala populations across Australia are on a rapid decline due to many culprits including habitat loss, being hit by cars, attacks by dogs, and the Chlamydia infection. Yes, that’s right, Chlamydia. And when koalas are brought into wildlife hospitals, they are treated with antibiotics to cure their Chlamydia infection. Although ridding koalas of Chlamydia, the antibiotics also kill off important gut microbes that are essential to the koala’s life biology. Koalas eat a diet solely of eucalyptus leaves, which would be poisonous to the koalas if it wasn’t for the tannin-protein-complex-degrading enterobacteria that break down the toxic components of the koala’s diet. Brace yourself, because the koala’s biology gets even more interesting! Mother koalas feed their young joeys a substance called pap, a fecal matter more concentrated in nutrients and microbes than normal feces. This form of a natural fecal transplant allows the joeys to colonize the critical gut microbes necessary for them to eat noxious eucaplytus leaves. But what does this mean for joeys whose mothers have been administered antibiotics?
My name is Katie Dahlhausen and I am A PhD student in Jonathan’s lab. I am crowd-funding a project to study this fascinating koala biology, as well as investigate alternative infectious disease treatment where antibiotics are not a viable option. Want to help out these adorable critters? You can support the Indiegogo campaign here, which is live until June 16, 2015. More information about the project is available on the crowdfunding page, and in these recent articles published in Scientific American and the Washington Post.
So how did I get into this project? Well, When I was at the Australia Wildlife Zoo in Australia last September, there was a sign next to the koala exhibit with picture of a joey whose mouth was covered in a brown substance. The sign read something like “It’s not chocolate!” and explained the pap part of the koala’s biology.
The moment I read this I knew there was some fascinating microbiology questions that were begging to be answered. While researching the microbiology behind this behavior, I found a study the recorded the detrimental effects antibiotics had on a koala’s eating habit and inability to maintain weight, but the question of how antibiotics were effecting the microbial composition of koala’s guts remained unsolved. That is how this whole project started. Like most people, I think koalas are cute and appreciate how iconic they are to Australia. Otherwise, I’m not very attached to koalas – they are actually quite mean and antisocial! But koalas are a fantastic model system – one food source, plenty of sampling opportunities (in Australia at least), frequently given antibiotics, and clear mechanism of the transfer of microbes from mother to offspring. The implications of the study are vast, but are aimed at the care for animals in captivity and foster changes in how/when we administer antibiotics.
Katie Dahlhausen, a PhD student in my lab, has become really really interested (perhaps a bit obsessed) with a really interesting case study regarding koalas, Chlamydia, antibiotics, and microbiomes. Since we do not have funds to work on this in the lab, she has started an Indiegogo campaign to raise funds to work on this. For more information on this project and how Koalas, Chlamydia, antibiotics and microbiomes are connected see “The Koala Project” page.
The UC Davis Pre-Health Student Alliance’s objective is to introduce and support academic, admission, and preparatory opportunities for all students interested in health professions with a focus on those underrepresented in healthcare (with regard to gender, economic, social, educational, linguistic, cultural, racial, and ethnic background). We target universities, community colleges and high schools throughout the United States. The UC Davis Pre-Health Student Alliance aims to impact health education, increase diversity amongst the healthcare workforce, and inspire future leaders of healthcare through hosting the largest national pre-health professions conference.
It was that mission statement that got me to ditch my wife and kids Sunday AM (and also much of Saturday PM for a dinner and to work on my talk). I went to a dinner Saturday for some of the speakers with the new Dean of the UC Davis School of Medicine Julie Freischlag. The dinner had about 20 or so people and I met some quite interesting folks there working on various aspects of human and animal health.
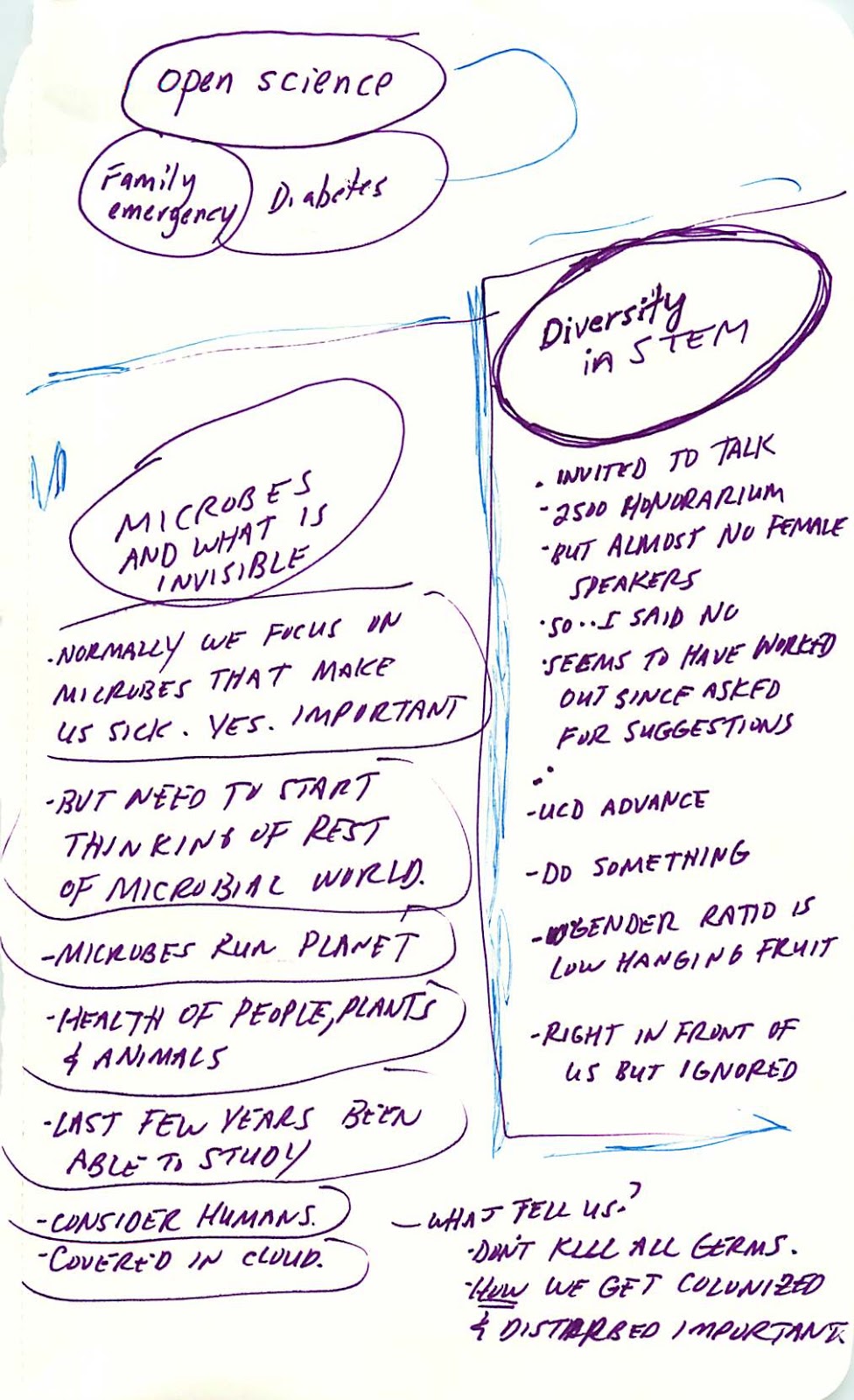
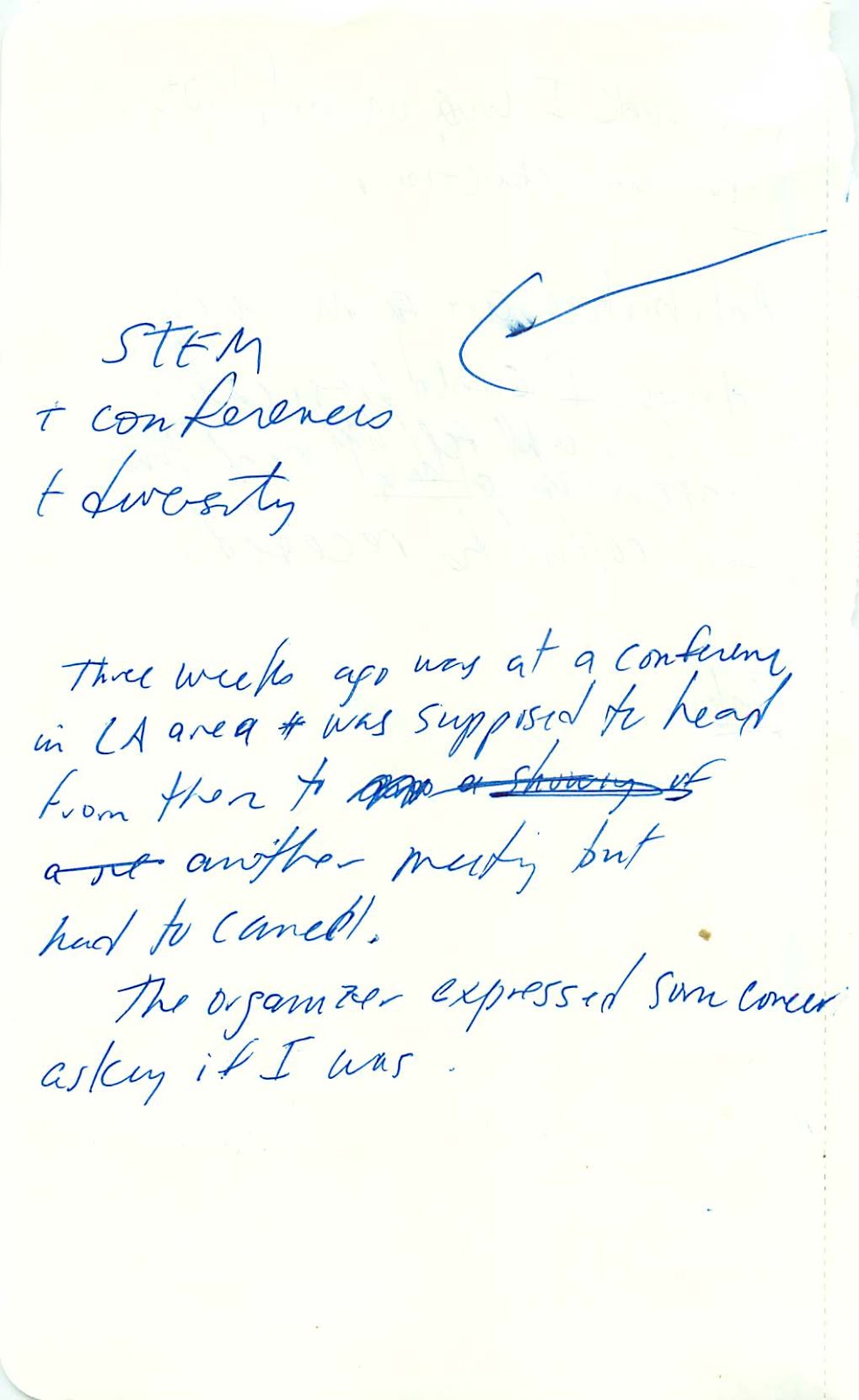
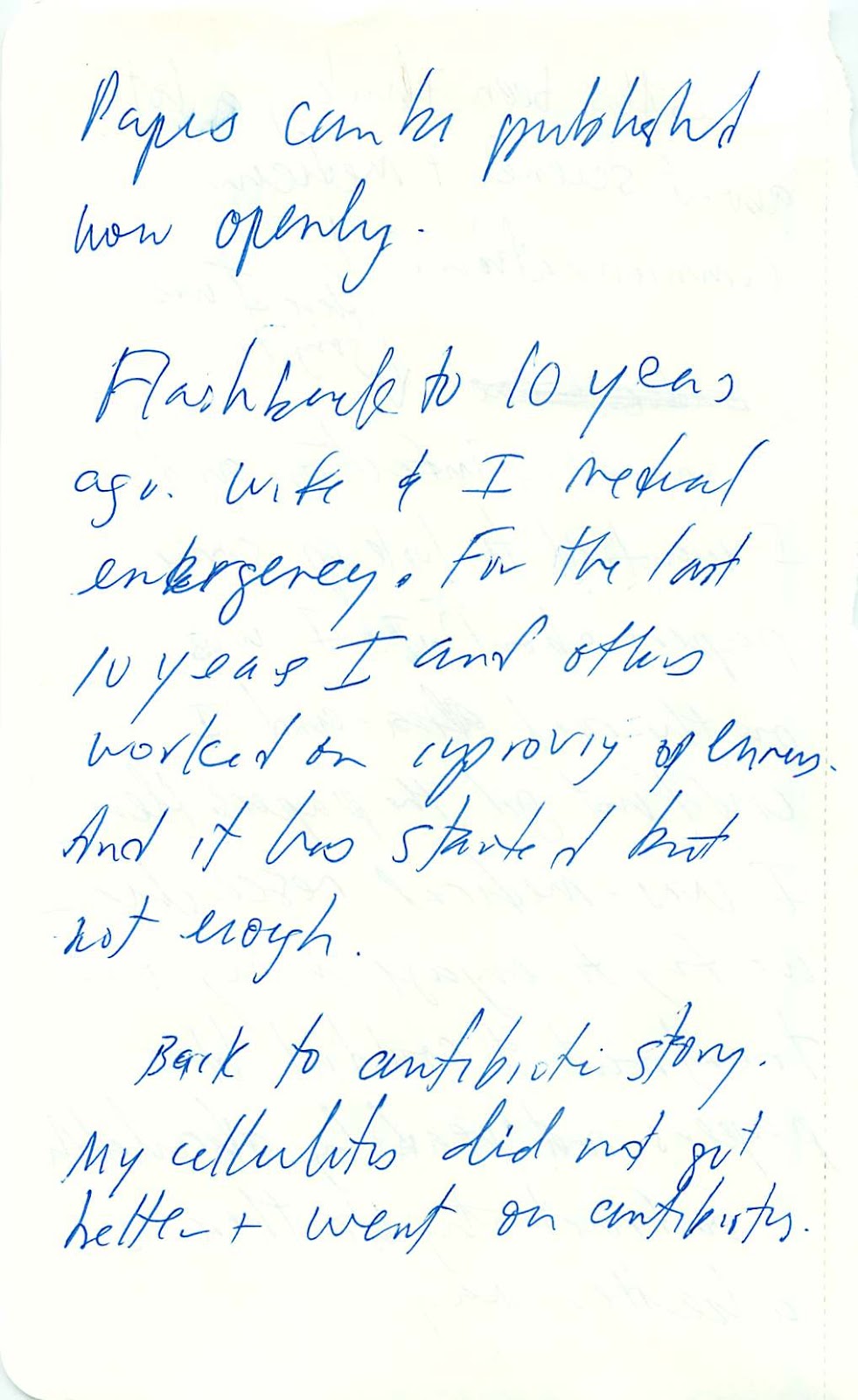
And then Sunday AM I got up early, decided to use slides (was not sure) and finished off the slide set I had worked on the night before. I decided that, in the spirit of the meeting, I would talk about two main things – diversity and access. And I planned to tell three stories about my work in this area. I wove in some personal stories since, at the dinner the night before Barbara Ross-Lee (who I sat next to) helped remind me of the importance of making talks personal. So in the end I talked about myself, diabetes, diversity of microbes, antibiotics, diversity in STEM, and open science. I came up with a title I was OK with: Opening up to Diversity.
My talk went well, I think. I am pretty sure it was vbideotaped but not sure where that recording will end up. I did however post my slides to slideshare. See below:
And I also recorded the talk using Camtasia (basically, it allows recording of the screen, the video camera on my computer, and the audio). I posted the recording (without the video feed which shows mostly my neck) to Youtube. See below:
UPDATE 10/16 –
I have scanned in my notes that I made in planning this talk. Figured, why not post them.
Update: 12/10/2014 – just discovered a video of the talk was posted to Youtube
The article starts of OK – reporting on the new WHO report on antibiotic resistance. But then it gets into the microbiome and what antibiotics supposedly do to it. Some quotes:
“But even more concerning, say experts like Dr. Martin Blaser, director of the human microbiome program at the New York University Langone Medical Center and author of Missing Microbes, is how these antibiotics are affecting the makeup of both good and bad bacteria that live within us – our microbiome. The first big cost of antibiotics is resistance,” he says. “But the other side of the coin is [the fact that] antibiotics are extinguishing our microbiome and changing human development.”
Extinguishing our microbiome? Really? The evidence simply does not support such a claim. I personally think antibiotics may be contributing to messing up the microbiome in many people and that this in turn might be contributing to the increase in a variety of human ailments (e.g., I mentioned this issue in my TED talk and many many times here and elsewhere). But “extinguishing”? Not even close. In fact, many of the published sutdies done so far suggest that the human microbiome is pretty resilient in response to antibiotics. Really serious overselling of the impact of antiobitcs by Blaser.
And “changing human development?” Not sure what the evidence for that is either. Most likely this refers to the role the microbiome plays in immune system development but I am not aware of strong evidence that antibiotics lead to changes in human devleopment.
They then quote Blaser again:
If I prescribe a heart medicine for a patient, that heart medicine is going to affect that patient,” says Blaser. “But if I prescribe an antibiotic, that antibiotic will affect the entire community to some degree. And the effect is cumulative.
Yes antibiotics can affect more than one person because microbes (and resistance) can spread. But “the effect is cumulative”? I do not think that has been shown.
Finally, Time (well, Alice Park, the author) states (in relation to limiting overuse of antibiotics)
That may also help to protect our microbiomes, which in turn could slow the appearance of chronic diseases such as obesity, cancer and allergies.
What? Now antibiotics cause obesity? And allergies? And cancer? Sure – there is good reason to think that antibiotic usage plays a role in obesity and allergies. The evidence is not yet completely overwhelming but it is certainly a reasonable notion. But how did cancer get thrown in here?
I note – as I assume many know – I think the microbiome is critical to many human functions and phenotypes. And screwing with it via excessive use of antibiotics seems like a very very bad idea. The precautionary principle says to me we should avoid any antimicrobials unless absolutely necessary. But do we really need to overstate what we know in order to effect change? Do we need to say things like “antibiotics are extinguishing our microbiome” which is simply untrue? I don’t think we do. I think we can be more careful, not mislead people, and still have an impact. And thus, I am giving out today’s “Overselling the microbiome” award to Time magazine and Martin Blaser.
Some papers that offer a more tempered view of the role of the microbiome in causing various disease:
CE West, MC Jenmalm, SL Prescott. 2014 The gut microbiota and its role in the development of allergic disease: a wider perspective. Clinical & Experimental Allergy, 2014
Disturbed gut colonisation patterns have been associated with allergic disease, but whether microbial variation is the cause or effect of these diseases is still under investigation. We are far from understanding what constitutes a “healthy gut microbiome” that promotes tolerance. This remains a major limitation and might explain some of the inconsistency in human intervention studies with prebiotics and probiotics. Multidisciplinary integrative approaches with researchers working in networks, using harmonised outcomes and methodologies are needed to advance our understanding in this field.
Such data suggest that bona fide associations may exist between microbiota and obesity in humans, although causality remains to be addressed. Whether these associations will hold up to large-scale replication has yet to be determined. This situation is reminiscent of genetic association studies done in the pre-genome-wide association scan era, during which many candidate associations were found using sample sizes which at the time were considered large, but were rather small in retrospect [54]. Very few of these earlier associations have held up to replication in the modern era, where the threshold for association is more stringent and requires sample sizes orders of magnitude larger [55]. It seems reasonable to postulate that causal contributions from the gut microbiome to the development of human obesity have effect sizes on the order of common genetic variations implicated in complex diseases. If this is the case, much larger studies will be necessary before we have clear evidence of association.
This review considers the nature of the evidence supporting a relationship between the microbiota and the predisposition to disease as associative, correlative, or causal. Altogether, indirect or associative support currently dominates the evidence base, which now suggests that the intestinal microbiome can be linked to a growing number of over 25 diseases or syndromes. While only a handful of cause-and-effect studies have been performed, this form of evidence is increasing.
Talk by Rob Knight on “From Correlation to Causation in Human Microbiome Studies”
Update 5/4 #2. I would also recommend people check out the Helicobacter foundation web site. which has some useful background information on the organism and the diseases it causes.
Update 5/4 #3. Some recent papers by Martin Blaser worth looking at
Oh – and Barry Marshall – winner of the Nobel Prize for discovering how H. pylori causes ulcers and cancer – chimed in on Twitter:
@phylogenomics@barjammar Jonathon, I never killed anyone by giving them antibiotics but I know of plenty who died when they didn’t get ’em. — Barry Marshall (@barjammar) May 3, 2014
Excellent suggestion of @TCNoel to discuss reasons for, against elimination of H. pylori in microbiology course http://t.co/y9P1yXtTDM — WvSchaik (@WvSchaik) May 1, 2014
A related question I have been thinking about involves Caesarian sections and whether they lead to an increased risk of any ailments that might have a microbial connection (e.g., obesity, allergy, autoimmune diseases). I started digging into the literature on this for my TED talk and then again when I posted something from the Smithsonian Genomics Exhibit that suggested there were no risks associated with C-sections.
Some papers on the topic suggest there may be some risks from C-sections related to these topics but that they are very very small:
And in at least a few of these stories, Martin Blaser’s book is referenced in relation to whether antibiotic usage may contribute to this. So one might ask – is there evidence for whether antibiotics contribute to type 1 diabetes? I think the results are unclear and ambigious. See some of these papers and stories:
I just can’t keep up. These seem like they might be worth reading. But no time to blog about them. So here are some possible things to look at if you care about obesity and its possible connection to the microbiome.
Am having a hard time right now with the comments from the authors of this new paper showing a correlation between H. pylori presence and both type II diabetes and blood glucose levels. As far as I can tell, the paper does not show any causal connection. That is, they do not determine if H. pylori infection is a cause of blood sugar issues or a consequence of blood sugar issues.
Yet the authors of the paper, one of whom (Martin Blaser) is a very respected H. pylori expert are saying things like
This to be seems to be a bit over the top. Yes, it makes sense that H. pylori could cause these issues. And they have a model for how it might. But they really should be more careful with their words until a causal connection is established. After all, we have many well known negative effects of antibiotic overuse, including some shown by Blaser. The last thing we need is people going out and dosing up on antibiotics in the hope that it will prevent type II diabetes. But I can guarantee that is what will happen if this story gets overplayed.
At least a few sources report on the lack of anything showing a causal connection (e.g. see US News and World Report):
An expert not involved with the study said that while it did not show a cause-and-effect relationship between the bacterium and diabetes, the findings suggest certain possibilities
But I am worried that that is not enough skepticism to counteract the claims of the authors here. The study is certainly interesting. And their model for a causal connection is fine. But they probably need to do a little bit of toning down of their claims here.
UPDATE: 3/17/13
After some people asked me questions about this study at a few recent meetings I dug a little deeper. And I am a bit startled to find out what the basis is for Chen and Blaser to claim a causative association between H. pylori and type II diabetes/ glucose levels. Here is a summary of their logic:
Helicobacter pylori is acquired almost exclusively in childhood [8], and there is no clear mechanism for how glucose intolerance present only after the age of 18 would increase risk of H. pylori colonization. It also is unlikely that H. pylori positivity and high levels of HbA1c levels share a mutual antecedent cause because there is no diathesis to both acquire H. pylori and to cause glucose intolerance.
They go on to discuss other lines of indirect evidence for why they think their conclusion is correct. And some of this is very suggestive. But “likely” and “suggestive” is not proof. There are many possible issues with their conclusion. In particular I think it is easy to come up with a scenario whereby something about the host (either their genetics or their history of exposure or even their micro biome) could influence both whether or not they get colonized by H. pylori or even whether or not they get colonized by particular strains of HP. And the same factor could influence microbiome interactions later in life. I see no evidence to indicate that H. pylori is the causative agent here. And for them to then basically recommend prophylactic antibiotics for elderly with HP seems dangerous at best.
Well, I have been out sick for a while. But I am now finally apparently getting better. Thanks to the work of scientists who have developed multiple classes of antibiotics. Anyway, more on that later. While I was out sick I spent a lot of time searching the web for information about nasty, cellulitis causing antibiotic resistant bacterial infections. And I was researching some other health related issues that may have contributed to my getting such an infection. Here are some tidbits I learned during this forced homecation.
Complete OA still a long way off. One thing I re-learned during this was that it is incredibly frustrating to see how much of the biomedical literature is still not freely available online. Shame on Elsevier and all the others who are still hoarding this important information.
Thanks to those providing OA. Related to the above issue, I came to appreciate was the societies and publishers have decided to go the OA route. I spent a lot of time reading material from ASM, BMC, PLoS, Hindawi, and a few others. And I am grateful to these groups.
Google rocks for science searching. Cuil, not so much. If you need to find something about some scientific concept or issue, Google really does a great job. While I was out, Cuil was announced as a possible new competitor for Google in searching. From my experience, Cuil is really really lame for science searches. I like their presentation in a magazine style. But the search results were not so good.
Anyway, enough about me. This is just a quick post to say the Tree of Life will be coming back over the next week or two. I am still out sick. But a clear sign to me that I am getting better is that I finally want to blog again.
Well, lots of researchers manipulate microbes in various ways in the lab. They delete genes. They make mutants They insert genes. Sometimes, they insert antibiotic resistance genes to help with the genetic manipulations they are doing.
Do researchers always think about the potential risks of what they are doing? Well, probably not. Most of the time that is OK as the risks are negligible. But some of the time, there are real risks to consider. One example of a real risk is the introduction into some pathogen of genes encoding a form of antibiotic resistance not seen normally in that pathogen. If that strain escapes from the lab, it could, in theory, spread into the real world and make treating infections by that pathogen more difficult.
All Things Considered had a very interesting story on “Making Drug-Resistant Germs In The Lab” about exactly this issue a few days ago where they discussed how one researcher submitted to an NIH oversight panel a request to carry out this type of experiment. It seems as though very few researchers actually submit requests to carry out these experiments, even though many are doing it. NPR also discussed how the CDC reviews requests to manipulate certain really nasty pathogens and that most of the requests have been granted. Unfortunately, I cannot find a transcript for this story to quote, but it is really worth listening to.
I find it sad that the world has come to this. The FDA announced that it has approved the use of viruses as a food additive. The particular viruses (known as phage in this case) target and kill common bacterial pathogens found in meat. It is entirely possible that this treatment will lead to reduction in deaths and illnesses. However, it is also possible that there will be unexpected consequences of this treatment and thus anything like this should be done with caution. What saddens me about this whole thing is that it is the wrong way to go about solving the problem. Most of the problem comes from the fact that our meat today in this country does not come to us in reasonable condition. The animals are usually kept in unsanitary conditions where diseases and nasty pathogens are prevalent.
The best way to think about this in my opinion is what I read in The Omnivore’s Dilemma, the new book by Michael Pollan. In this book he talks about how animals now frequently live in what can be considered the equivalent of the slums of the industrial revolution. Cities of animals, frequently wallowing in excrement, is not the best way to prevent bad microbes from getting in our food.
So in recent years all sorts of practices have been developed to kill these microbes in food products. Irradiation, for example. And now, viruses, sprinkled on your meat, to keep the bacteria from growing too much. Give me meat from animals that have not been swimming in their own shit and piss and I will be happy to take my risks without dumping viruses on top.